|
| Guess What! - ESTP Case 28 |
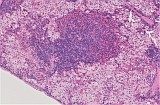
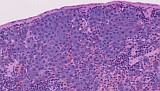
The lesion (Figures 1–4) was observed in the spleen as an incidental finding in a male A/J mouse which was sacrificed at the end of a long term study. Cells of similar appearance were found isolated or in very small clusters also in the liver (Fig. 5).
| Click on the images below for a larger view. |
|
Fig. 1: Spleen. H&E, magnification 2.5x
|
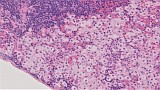
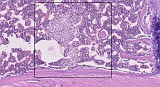
Fig. 2: Higher magnification, H&E, 10x
|
|
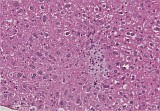
Fig. 3: Higher magnification, H&E, 20x
|
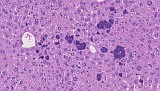
Fig. 4: Higher magnification, H&E, 40x
|
|
Fig. 5: Liver, H&E, 40x
|
For case 28 we have received 9 responses. Five of the participants suspected an increased number of macrophages or histiocytes in the red pulp of the spleen and in the sinusoids of the liver. For some of them it appeared as if the cells would contain some vacuolation and therefore thought it could be a lysosomal storage disorder or named it directly phospholipidosis. The cells were described as containing abundant clear cytoplasm with small sometime confluent vacuoles by one respondent while another person characterized them as having a high cellular differentiation with low pleomorphism, low mitotic rate and showing no nuclear abnormalities such as multinuclearity or heterochromasia. However, the apparent uniformity of the cells with a clearly centrally located nucleus makes it rather unlikely that they represent a macrophage origin.
Three colleagues called the lesion a mast cell tumor, a fourth one named it mastocytosis, the direction which was hoped for. One answer described the lesion very precisely: Neoplastic cells look round to slightly oval, with pale, finely granular, abundant cytoplasm with no specific tinctorial affinity and a single centrally placed, round to oval, euchromatic nucleus with a small single basophilic nucleolus. Among the submitted diagnoses, it was suggested to support the diagnosis with special stains such as Giemsa or Toluidine Blue or Astra Blue to confirm cytoplasmic metachromatic granules. Alternatively, it was proposed to use IHC for the detection of mouse mast cell protease. Unfortunately, no possibility was given to perform any of the named special methods. Nevertheless, we strongly believe that the presented case represents a mast cell lesion and appreciated a comment from one participant who suspected that the cells maybe stemming from a poorly-granulated mast cell or from a mast cell subcategory that doesn’t stain properly when fixed with formalin (like mucosal vs connective tissue mast cells). Recently, we observed another case in the same strain of mice showing similar features. However, this time the cytoplasmic granules were more prominent, especially in the liver where they occurred more abundantly (new figures). In contrast, the accumulation of cells in the bone marrow of the sternum appears as pale as in the presented case.
The main problem with the presented lesion is its naming and assessment. The INHAND fascicle published in 2019 on the proliferative and non-proliferative lesions of the hematolymphoid system of the rat and mouse (Tox Pathol 47, 665-783) provides a descriptive, conventional and enhanced terminology for this kind of lesions. Increased cellularity of mast cells (descriptive term) or the conventional term mast cell hyperplasia are described as a loosely arranged collection of mature mast cells without nodule formation with no compression of adjacent tissues which may occur in one or more tissues or organs. Does this include the bone marrow for which it is said that the malignant variant of a mast cell tumor does not occur? Depending on the type of fixation, the cytoplasmic granules may be visible or not with hematoxylin and eosin. Granules are not visible in the present case which does not exclude the diagnosis. Also, there is no clear compression of the adjacent tissue but the question is, whether the pronounced accumulation of cells may be seen as a "nodule". A single, solitary, compact (dense) aggregate, or nodule would be considered as a tumor, mast cell, benign. In the present case, we see a "compact aggregate", but also loosely scattered mast cells in other areas of the spleen. Moreover, it is said, that there should be no systemic involvement but we observe similar cells in the liver and also in the bone marrow of a second case (new picture). The description for the systemic type of tumor mast cell, malignant with compact nodular or sheet-like accumulation(s) of round, spindle-shaped, or immature mast cells, present in at least two organs would fit for the present case. For this kind of lesion, it is also said that the cytoplasm appears frequently hypogranular, however, the description excludes the presence of tumor cells in the bone marrow.
Another possibility to name the lesion would be to call it leukemia, mast cell. This entity is described as a presence of atypical mast cells in the liver, spleen, bone marrow and/or peripheral blood which show a sheet-like or leukemic pattern in one or more hematolymphoid organs. In the additional case (new pictures), we have a presence in all the named organs but none of the cells have to be considered atypical. But indeed, the liver, which regularly is not primarily called a hematolymphoid organ in the adult mouse but has the capability to function as such (Sakomoto T et al. 1992, Reg Immunol 4, 1-11) shows a clear leukemic pattern. Thus, mast cell leukemia would be our preferred diagnosis.
Mast cell tumors in mice are considered as rare events. In the RITA data-base there are only single events recorded. Only one benign mast cell tumor has been observed as a single nodule in an extraorbital lacrimal gland in a 756 days old female CD1 control mouse. Malignant mast cell tumors have been found in 10 among approximately 10.000 cases, some of which probably have to be reclassified since a benign variant has not been determined before (Mohr, U. 2001, International Classification of Rodent Tumors: The Mouse) and was only recently introduced with the new above mentioned INHAND fascicle.
To conclude and as is pointed out in the recent INHAND comment: Little is known about mast cell proliferations in rodents and the terminology for proliferative conditions is confusing. The classification presented here is proposed as a standardized terminology for use by the toxicologic pathology community. This classification is considered a work in progress and changes are anticipated as knowledge and understanding of rodent mast cell proliferations evolve. Case 28 was intended to support on this way.
| Click on the images below for a larger view. |
|
Fig. 6: Mast cells (atypical, leukemic) in liver
|
Fig. 7: Mast cell nodule in spleen
|
|
Fig. 8: Mast cells in spleen, higher magnification
|
Fig. 9: Mast cells in sternal bone marrow
|
|
|