|
| Guess What! - ESTP Case 25 |
Introduction
Case 25 was on the website for more than a year but only five responses were received despite several reminders to participate and give an opinion. It showed a variety of non-proliferative and proliferative changes in the adrenals of an aged male mouse of the CD-1 strain, which reached the terminal sacrifice after being two years being employed in the study. This case was chosen to point out the challenges that may evolve during the evaluation of the adrenals from aged animals from carcinogenicity studies.
In fact, it was put to the website before the INHAND fascicle on the Endocrine System was available. One contributor mentioned that it was difficult to make diagnoses since the resolution was not good enough. This is admitted and we therefore describe the lesions here in a separated form and attach according illustrations.
Histological Features
The adrenal gland of the mouse shows several features which differ from other species: Only the zona glomerulosa can be distinguished from the zona fasciculata even though they are not sharply demarcated from each other (Braendli-Baiocco et al. 2018). While the glomerulosa cells are small and arranged in indistinct arches, the more eosinophilic fasciculate cells are arranged in columns. In young animals they make up about 70% of the cortex (Nyska and Maronpot 1999). This changes with age. Even in young mice distinction between the different zones of the adrenals is arbitrary and a clear differentiation between fasciculate and reticulate zones (if there is any) is not possible.
Unique to the mouse is the X-zone, the function of which is still not clearly understood. While in males it regresses during puberty (post-natal week 5) it reaches is maximum in females at an age of approximately 9 weeks. In aged mice it does not play a role but certain cells located between cortex and medulla may represent remnants of this fetal and postnatal zone. Another feature especially of the male mouse is the presence of subcapsular cells, which occur in the spindloid A and the B cell type.
In the literature, there is inconsistent information about the amount of medullary tissue: INHAND states that the medulla makes up about 10% of the total adrenal tissue in rodents (Braendli-Baiocco et al. 2018) but does not differentiate between mice and rats. Nyska and Maronpot (1999) say that the medulla comprises about 20% of the adrenal tissue volume in B6C3F1 mice. The medulla is composed by irregular packets of polyhedral chromaffin cells and ganglion cells along with a rich vascular structure of venules and capillaries. Based on staining reactions and ultrastructural features there are two types of chromaffin cells: epinephrine and norepinephrine secreting cells of which the epinephrine secreting cells represent 85% of the medulla (Tischler and Sheldon 1996).
| Click on the images below for a larger view. |
|
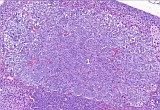
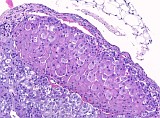
Fig. 1: Adrenal of a male CD1 mouse
|
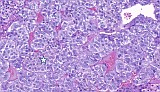
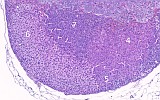
Fig. 2: Adrenal of a male CD1 mouse
|
|
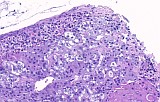
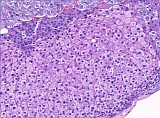
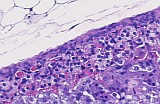
Fig. 3: [1-1] Adrenal Medulla: Focal Hyperplasia showing an area of increased number of nuclei and tinctorial difference, but no compression. Since the size is also less than 50%, the lesion is not yet considered as a phaeochromocytoma
|
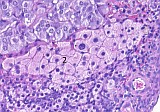
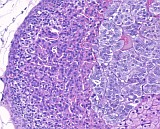
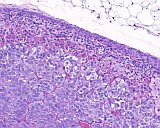
Fig. 4: [2-1] Normal medulla. Note the slight tinctorial difference of epinephrine and norepinephrine (asterisk) producing chromaffine cells that occur in a relation of approximately 85:15%.
|
Fig. 5: [1-2] Cortical hypertrophy with nuclei of variable size
DD: Hyperplasia, focal but no indication of increased cell number
|
Fig. 6: [2-2] Normal adrenal medulla at the hilus
DD: Subcapsular Type B-cells or Macrophages
|
|
Fig. 7: [1-3] Subcapsular cell hyperplasia, Type A with some intermingled Type B-cells (?). Diffuse distribution rather than nodular appearance. No bulging of the surface.
|
Fig. 8: [2-3] Cortical Hypertrophy: No increase in number of cells, marked eosinophilic partly condensed cytoplasm (formerly called eosinophilic focus), still somewhat arranged in columns, though showing compression
|
|
Fig. 9: [1-4] Focal cortical hyperplasia: Increased number of cells, altered architecture, only slight compression, smaller than width of the cortex, thus not yet considered as an adenoma
|
Fig. 10: [2-4] Relatively normal adrenal cortex (Z. fasciculata)
DD: Slight Cortical Hypertrophy
|
|
Fig. 11: [1-5] Focal cortical hyperplasia with even more increased number of nuclei, probably part of 4
|
Fig. 12: [2-5] "Reserve" cells? Hyperplasia of fetal (X-zone) cells?
|
|
Fig. 13: [1-6] Normal cortex (Z. fasciculata) with slight cortical hypertrophy at the edge: Cells are still arranged in columns
|
Fig. 14: [2-6] Focal cortical hyperplasia: Increased number of cells/nuclei but no spindloid appearance, i.e. no downgrowth of subcapsular A-cells.
OR focal atrophy of fasciculata cells since there is no compression
|
|
Fig. 15: [1-7] Debatable: Hyperplasia of fetal cells (X-zone) or cortical hyperplasia ?
|
Fig. 16: [2-7] Cortical Atrophy: Normal capsule and zona glomerulosa cells but nearly no fasciculata cells. Medulla appears normal at the edge and shows no diffuse proliferation or compression
|
|
Fig. 17: [1-8] Cortical Atrophy: Normal capsule and zona glomerulosa cells but nearly no fasciculata cells. Medulla appears normal at the edge and shows no diffuse proliferation or compression
|
Description of Findings and Differential Diagnoses
In the presented case, the overall size of the adrenal glands seems not to be altered, thus a space-demanding neoplastic proliferation is unlikely (Overview Fig. 1 and 2). However, the amount of medullary tissue seems to be much more than described in the literature, probably due to the marked atrophy of the cortical fasciculata cells (Fig. 1-8, 2-7). A closer look to the medulla (Fig. 1-1) reveals that there is a hyperplastic area of increased number of nuclei and tinctorial difference, which however, shows no compression to the surrounding cells. Since the size is also less than 50% of the medulla, the lesion is regarded as focal medullary hyperplasia and not yet considered as a pheochromocytoma as it was diagnosed by one contributor. The medulla of the other adrenal seems to be without any change (Fig. 2-1). Fig. 2-2 represents normal medullary cells at the hilus rather than macrophages or subcapsular B-cells.
Capsule and zona glomerulosa seem to be free of any major alteration. Circumscribed normal cortical (zona fasciculata) tissue is seen in Fig. 1-6 and 2-6. Focal cortical hypertrophy characterized by pale and enlarged cells with enlarged nuclei can be found in Fig. 1-2. Another feature of focal cortical hypertrophy composed of large eosinophilic cells is shown in Fig. 2-3. Since the cells are still arranged in a columnar pattern this lesion is not regarded as a neoplasm.
Fig. 1-4, 1-5 and 2-6 might represent bilateral focal cortical hyperplasia, being tinctorial different. There are more nuclei per area and the columnar architecture is no longer preserved. There is also only little compression of the surrounding tissue. However, they are smaller than the width of the cortex from a young mouse, which distinguishes this lesion from an adenoma. The descriptive terms "eosinophilic" and "basophilic" focus are no longer used according to the recent descriptions in INHAND. A debatable alteration is shown in Fig. 1-7 (and 2-5). Located in the X-zone it might represent a proliferation of fetal cells but could be also considered as an additional cortical hyperplasia.
Subcapsular cell hyperplasia is shown in Fig. 1-3. Since it does not bulge the surface or causes compression at any place it is regarded as a diffuse rather than a focal lesion.
References
- Braendli-Baiocco A et al. (2018) Non-proliferative and proliferative lesions of the rat and mouse endocrine system. J Toxicol Pathol 31 (3Suppl): 1S-95S
- Nyska A, Maronpot RR (1999) Adrenal Gland. In: Maronpot RR, Boorman GA, Gaul BW (eds) Pathology of the mouse. Reference and atlas. Cache River Press, Vienna, 509-536
- Tischler AS and Sheldon W (1996) Adrenal Medulla. In: Mohr U. et al. (eds) Pathobiology of the Aging Mouse. ILSI Press, Washington DC, 135-151
|
|